“Changing landscapes of Myeloma Treatments And The Role of Haematopoietic Stem Cells Transplantations, In the era of Targeted and Immunotherapy”
BICC 2019 DHAKA updated
80 years old lady was admitted via emergency department with increasing shortness of breath and cold fingers. she has no past medical history. Not on any medication Evaluation in the emergency department revealed only acrocyanosis . Her saturation were unobtainable via pulse oxymetry. System examinations were unremarkable emergency blood test are as below CHAD Film HB 43 MCV 127 (Significantly raised- normal range 82-95 ) WCC 12 , Neutrophils 7, Lymphocytes 5, CRP 100. Bilirubin 45, Creatinine 100 LDH 1200 Raised (Normal range 120-450) CXR : NAD Blood film examination showed roulaux formation http://janaanhealth.org/wp-content/uploads/2019/01/CHAD-Film.pptx Haematology team were contacted Direct antiglobulin test IGM +4 CD3d positive A diagnosis of Cold agglutinin disease were made CHAD Mainly idiopathic underlying LPD or rarely viral /bacterial infection usually refractory to Steroids unlike Warm autoimmune haemolytic anaemia Management look for underlying cause cold avoidance trial of prednisolone 1mg/kg may need CD20 antibody Rituximab or treat in underlying LPD Full antibody test at NHS BT Virology Folic acid life long 5mg po od there are case report of success with Eculizumab and Valcade in refractory disease under clinical trial
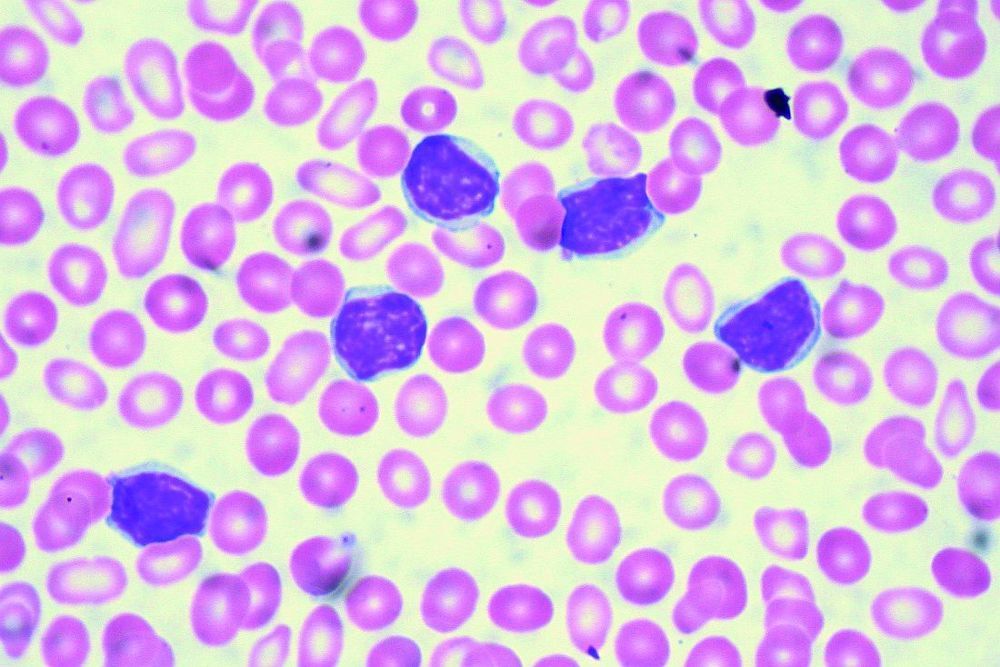
AML Blood film 64 years old lady presented to emergency department with history of coffee ground vomiting and being unwell. She had emergency resuscitation and appeared to be unwell . her vital signs were all stable apart from Pyrexia of 38.4 C. Blood pressure : normal Examinations were all unremarkable apart from bibasal crackles on both lower bases Her urgent blood test results were HB 64 WCC 360 PLT 172 CRP 389 high Uresa : 10, Creatinine : 98 (upper limit of normal) Full clotting screen : all Normal She was transferred to a ward and a haematologist on call were contacted she had emergency blood film as per Laboratory criteria which were looked at by biomedical scientist: suggested Acute myeloid leukaemia with over 90% myeloid blast initial management: 1,DO NOT TRANSFUSE 2,Patient is at risk of Leuckostasis 3,Exclude APML (Auer rods on film) 4,Full clotting screen (This patient has risk of DIC) Emergency transfer to the tertiary facility where emergency leukopheresis can be done Phone haematology consultant is the most important point of this patient care and should take emergency steps
18th October 2017 Marygreen Manor Hotel 128-130 London Rd, Brentwood CM14 Funded by ROCHE products limited

56 years old gentleman has had 6 hours history of non specific chest pain , it was thought to be releated to stomach ache initially. As the pain was getting worse he was taken by his son to a clinic in town for test and evaluations around 12 noon the next day , the attending laboratory technician did the basic bloods tests and the ECG but needed a reporting physician to come and report it later in the evening. which happened around 7 pm He was then advised for an emergency admission to either in a governement medical college hospital or a private fascilities for urgent treatment as he had a heart attack , advised by the doctor who reported the ECG. The attending son who is a 2nd year university student started paniking and decided to take his father to a local clinic to get quicker assessments He was admitted to this local clinic around 9 pm, he was commenced on basic pain kilers and iv fluids, his chest pain was getting worse and worse. The busy physician who was on his to clinic only arrived around 2 am in the next morning to complete his busy day schedule. By this time the patients condition has deteriorate and he was informed that his chances of survival is very slim , he had a massive heart attack, with low blood pressures and wowful ECG traces on monitor. A decision has been made by the family to take him to a […]
© Copyright 2017. Janaan Health. All rights reserved.